This is an online E log book to discuss our patients deidentified health data shared after taking his/her/guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE PRESENTATION:
A 70 year old male patient who collects toddy from tree came with C/O SOB since 3 months.
Patient was apparently asymptomatic 1 year back then he had H/O fall and pelvic bone # , was operated for that and was on bed rest for 7 months.Later, 3 back back he developed SOB grade IV, was taken to local hospital, due to high serum creatinine informed the need for dialysis but patient attendars requested medications to relieve symptoms as there was a family function.So they used adviced medications and his symptoms got relieved.Again 1 month back he developed SOB grade IV for which he was taken to hospital and since then he was on dialysis.Till date 9 dialysis in the span of 1 month were done.Recent dialysis was on 28/12/2020 during which he developed fever,high BP recorded and SOB and was shifted to ICU , later patient had cardiac arrest and revived with cpr.
On 1st of January till evening 100mg lasix infusion was given over 5 hours
Even with high flow oxygen saturation’s are falling to 70%
Patient was put on intermittent BIPAP overnight.
Saturation’s on BIPAP are 100%
K/C/O HTN since 15 years and DM since 15 years on medications.
No H/O TB,Asthama,CAD, Epilepsy,No H/O any previous surgeries.
Mixed diet, Normal Appetite, Bowel and Bladder regular.Chronic H/O Smoking and Alcohol consumption since 40 years.
General examination:
patient is conscious, coherent, cooperative moderately built and nourised.
Pallor +,Pedal edema +,No Icterus,Cyanosis, Clubbing, lymphadenopathy,
Vitals :
Temp -102 F,
BP : 150/90mmHg, PR-130bpm,
RR-26cpm,
SpO2 - 87 %@room air.




CVS : S1 S 2 Heard,No murmurs.
RS : BLAE +,NVBS +
P/A : soft,non tender
CNS : NAD
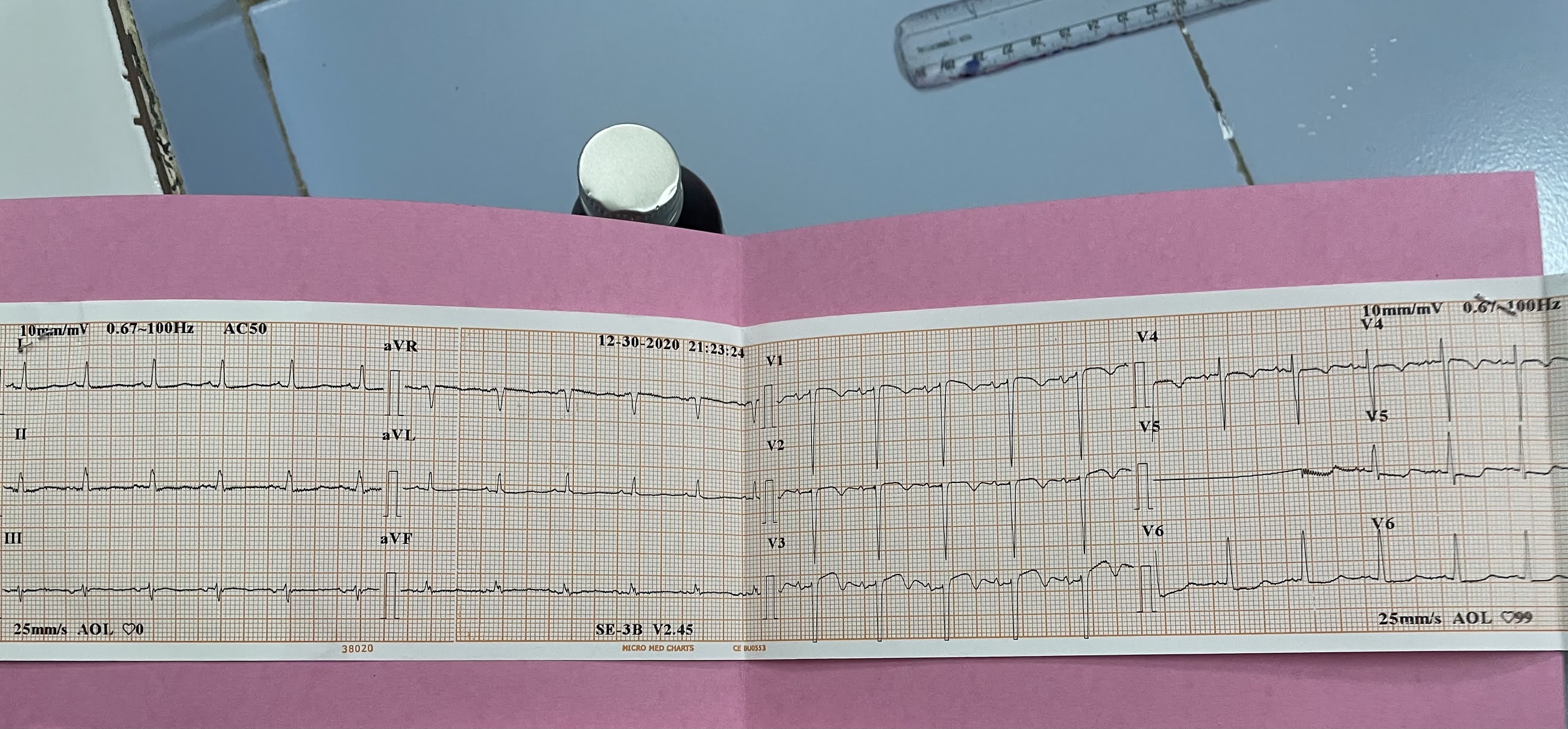
INVESTIGATIONS



DIAGNOSIS
CKD on MHD
DCMP secondary to CAD (LAd,RCA,LCX hypokinesia)
HFrEF(EF 40%)
? Cardiogenic pulmonary edema
B/L consolidations
Treatment
Salt restriction less 4g per day
Fluid restriction to 1L per day
Tab LASIX 40mg Po/TID
Tab NODOSIS 500mg Po/TID
Tab CLINIDIPINE 10mg Po/BD
Inj HAI according to sliding scale
Tab OROFER XT PO/BD
INJ AUGMENTIN 600mg Iv OD
Tab AZITHROMYCIN 500mg PO OD
TAB SHELCAL CT PO BD
TAB ALPHA D3 po OD
INJ ERYTHROPOIETIN 4000 IU SC WEEKLY ONCE
INJ IRON SUCROSE 100mg IN 100ml NS IV Weekly once.
SYP CREMAFFIN 10ml PO TID
RTPCR for COVID 19 was done in view of hypoxia
Reports were positive for COVID 19

Comments
Post a Comment