Acute on chronic pancreatitis
This is an online E log book to discuss our patients deidentified health data shared after taking his/her/guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE PRESENTATION:
A 35 year old male patient chef by occupation came with chief complaints of 5 episodes of vomitings on 4-1-2021 morning followed by pain in left hypochondrium, lumbar region, and left chest.
Vomitings : Non bilious , non blood stained , and food particles as contents.
Pain in left hypochondrium and lumbar radiating to left chest and right side of abdomen which is dull aching type.
No history of loose stools or constipation.
No H/O fever , cold , cough.
No H/O headache, loc , involuntary movements.
No other complaints.
H/O similar complaints in past ( every year from 4-5 year's) He is a k/c/o pancreatitis
K/c/o Hypertension from 2 years and on medication
TAB AMLODIPHINE 5mg
TAB ATEN 50mg
K/c/o Epilepsy
First episode was 10 years back
Sudden onset of involuntary movements of B/l upper and lower limbs associated with tongue bite , loss of consciousness. Unrolling of eyes present. Episode lasted for 10-15 min. No involuntary micturition or defecation.
He was taken to hospital immediately. Gained consciousness after 2 hours. Post ictal confusion lasting for 1 hour.
Last episode 8 months back.
Patient is on medication
Tab . PHENYTOIN 100mg OD
Patient is non compliant to medication.
Not a k/c/o DM, TB, Asthma,CAD.
Personal History:
Decreased appetite
Diet-mixed
Bowel and bladder regular
Chronic alcoholic from 20 years ( 15units every day )
Chews ghutka from 20 years ( 20 packets per day)
General Examination:
Patient is conscious coherent and cooperative
Moderately built and nourished
Icterus present
No pallor,cyanosis,clubbing,lymphadenopathy, pedal edema.
Vitals
Temp : 98.6F
Pulse Rate : 80bpm , regular
BP : 130/70 mmHg
RR: 20cpm
Systemic examination:
P/A : obese , tenderness present in left hypochondrium and lumbar region.
CVS : S1 S2 heard , no murmurs
RS : BAE +
CNS :
Motor examination
reflexes:
rt. lt
biceps. +2. +1
triceps. +1. +1
supinator +2. +1
knee. +2. +1
ankle. +2. +1



Psychiatry referral done I/v/o alcohol dependence.





Investigations:




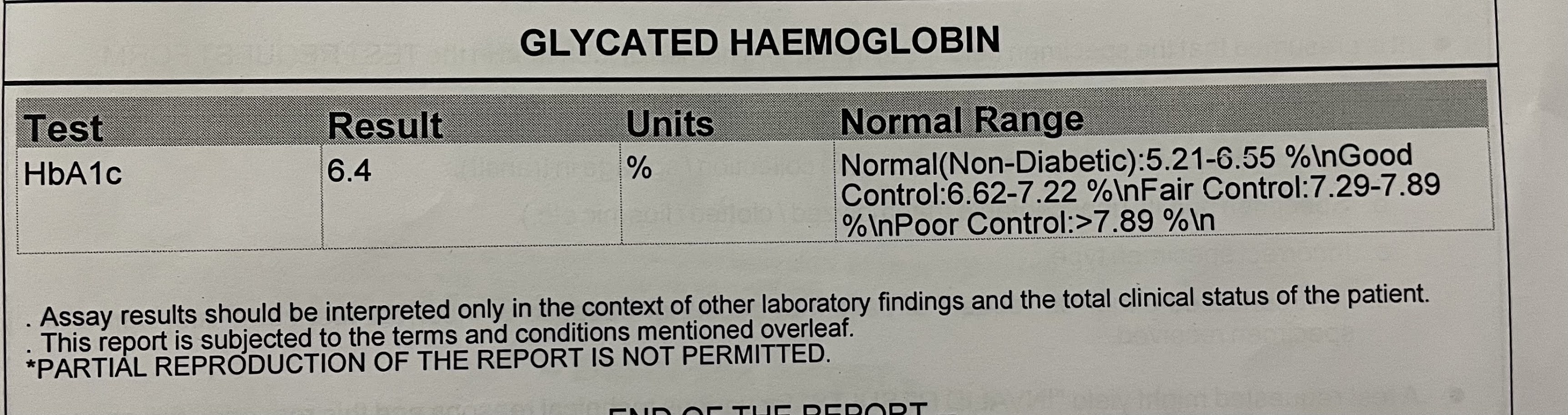








DIAGNOSIS:
? Acute on chronic pancreatitis.
Treatment:
IVF NS and RL @ 100ml /hour
INJ PANTOP 40mg IV OD
INJ ZOFER 4mg IV OD
INJ TRAMADOL IN 100ml NS sos (iv)
INJ THIAMINE 1AMP in 100ml NS iv TID
TAB EPITOIN 100mg PO OD
TAB ATEN 50mg PO OD
TAB AMLONG 5 mg po OD
TAB PREGABA M 75 mg OD
TAB LORAZEPAM 2mg 1-x-2 for 2 days
NICOTEX GUMS 2mg TID , SOS

Comments
Post a Comment