This is an online E log book to discuss our patients deidentified health data shared after taking his/her/guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE PRESENTATION:
A 36 year old male who is farmer by occupation and resident of Koch behar , West Bengal came with chief complaints of lower back ache with pain radiating to right lower limb since 20 days.
Patient was apparently symptomatic 20 days back then he developed sudden pain in the lower back with pain radiating to right lower limb, associated with calf pain.
H/o massage done 20 days back ( in view of pain in the right lower limb which was aggravated after that) , then he went to a near by RMP for medication (pain was relived by that medication ) . Pain was aggravated on on walking and relieved be rest.
History of surgery in March 2020
Surgery- L5-S1 right fenestration and discectomy under general Anesthesia.
Not a known case of DM , HTN , TB , Epilepsy.
Not on any medication.
Personal history:
Appetite normal
Diet mixed
Bowel and bladder regular
Sleep adequate
Chews tobacco.
General examination:
Patient is conscious coherent and cooperative.
No pallor icterus cyanosis clubbing lymphadenopathy edema.
Vitals
Temperature 98.6F
Bp : 120/80mmHg
PR: 84bpm
RR: 16cpm
GRBS: 112
Systemic examination:
CVS : S1 S2 heard , no murmurs
RS : BAE +
P/A : soft non tender
Leg raise test
Right 60 degrees
Left 90 degrees
CNS :
Higher mental functions normal
Speech normal
Memory intact
Motor examination
Power. R. L
UL. P 5/5 5/5
D 5/5 5/5
LL. P 4/5 5/5
D 4/5 5/5
Tone UL normal
LL normal
Reflexes B T S A K P
R 2+ 2+ 2+ 3+ 3+ Withdrawal
L 2+ 2+ 2+ 2+ 2+ Extension
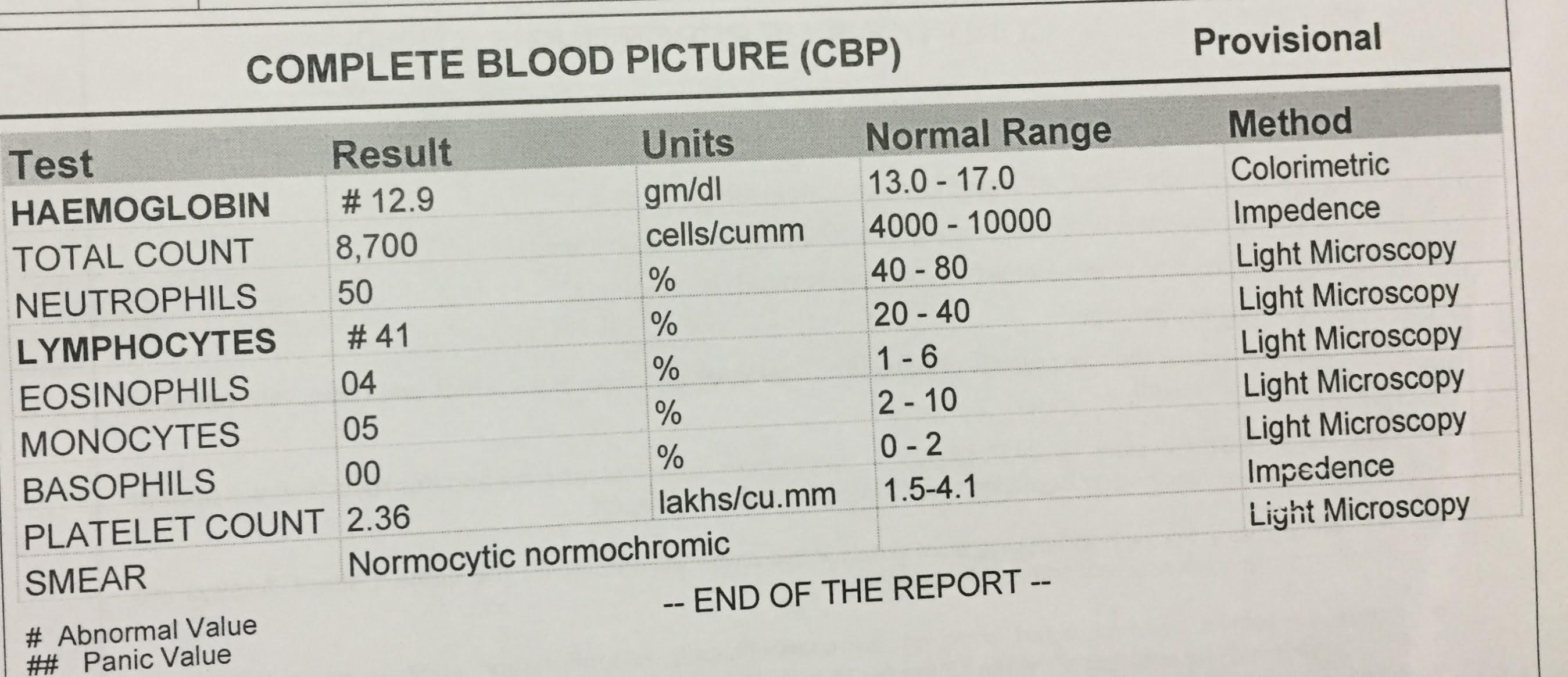
Investigations:














Comments
Post a Comment